MEDCINE FINAL PRATICAL(LONG CASE)
Hall Ticket No: 1701006156
Batch -2017
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan
55 years old female with shortness of breath
Chief complaints:
55 years old female who is housewife came to the hospital on 10th June,2022 with chief complaints of
-Shortness of breath Since 2 days
-Bilateral pedal edema since 2 days
-Decreased urine output since 2 days
TIMELINE OF EVENTS:-

HISTORY OF PRESENTING ILLNESS:-
No history of blood transfusions.
Personal history:
Diet -mixed
Appetite -normal
Sleep -adequate
Bowelmovements-regular
Bladder movements-decreased urinary output since 2days
No known drug or food allergies
No addictions
Family history:
No significant family history
General examination:
After taking consent ,patient is examined in well lit room
Patient is conscious, coherent and cooperative well oriented to time ,place and person
moderately built and moderately nourished
Pallor -present
Icterus -absent
Clubbing -absent
Cyanosis -absent
Generalised lymphadenopathy -absent
Edema - present

Temperature-afebrile
Pulse rate -106 beats per minute ,regular rhythm ,normal volume,normal character ,no radio radial delay
Blood pressure -160/80mmHg measured in left arm in supine position
Respiratory rate -34 cycles per minute
SpO2- 92 %at room air
Video showing pitting edema

Systemic examination:
Respiratory system:
Upper respiratory system - normal
Examination of chest-
Inspection:
Shape of the chest -normal, bilaterally symmetrical
Trachea -central in position
Respiratory movements -normal, bilaterally symmetrical
No scars,sinuses, engorged veins seen on chest wall
Palpation:
No local rise of temperature
No tenderness
All inspectory findings are confirmed
Trachea -central in position
vocal Fremitus - normal
Chest movements - normal ,symmetrical bilaterally
Percussion:
Resonant note heard
Auscultation:
Bilateral air entry present
Normal vesicular breath sounds heard
Bilateral basal crepitations heard
Diffuse wheeze present
Cardiovascular system:
Abdominal examination:
Inspection-
Shape of the abdomen- scaphoid
Umbilicus -normal
All quadrants of abdomen area moving normally
Palpation -
No local rise of temperature
No tenderness
Soft ,non tender
Liver not palpable
Spleen not palpable
Kidney not palpable
Auscultation -
Bowel sounds heard
Central nervous system examination-Investigations

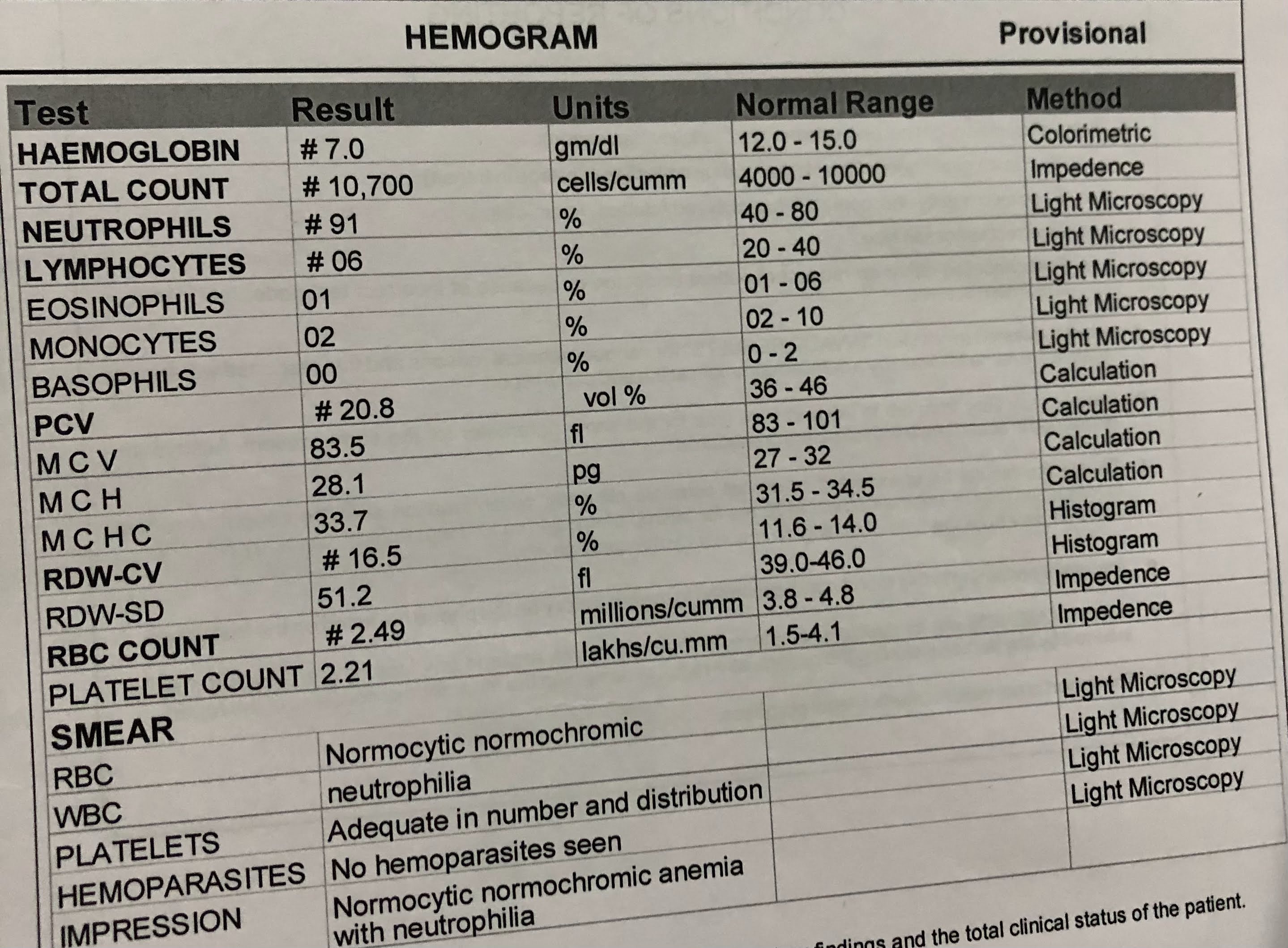
Complete blood picture-








Serum creatinine- 7.1mg/dl


APTT-

Urine for ketone bodies-





Ultrasonography -
Right Grade 3 RPD
Left Grade 2 RPD

1)Inj.LASIX 40mg IV/BD
2)tab.NODOSIS 500mg PO/OD
3)tab.MET-XL 25 mg OD
4)tab.AMLONG 10mgOD
5)cap bio-D PO weekly once
6)tab. SHELCAL 500 mg PO OD
7)inj. Erythropoietin 5000 units weekly once
8)inj.INSULIN SC according to the GRBS


12/06/22

fasting blood sugar





